Clinically reviewed by Dr. Ponlawat Pitsuwan, Physician, Doctor Bangkok. Last reviewed: July 2026
No, pseudogout and gout are not the same condition. Both cause sudden, painful joint swelling, but they are triggered by different types of crystals and affect different joints. Gout responds to urate-lowering treatment. Pseudogout does not. Getting the right diagnosis changes everything about how you treat it.
You woke up with a swollen, hot, painful joint. Maybe it is your knee. Maybe it is your wrist. You searched online and gout kept coming up. But something does not quite fit. The pain is not in your big toe. Your uric acid came back normal. You have been cutting out beer and shellfish for weeks and nothing has improved. This is one of the most common stories I hear from expats coming through the clinic.
The confusion between gout and pseudogout is real, and it matters. If you are being treated for the wrong condition, you will not get better. Both conditions feel similar in the moment, but they have different causes, affect different joints, and need different treatment. Here is what you need to know.

Quick Answer: No, But They Are Easy to Confuse
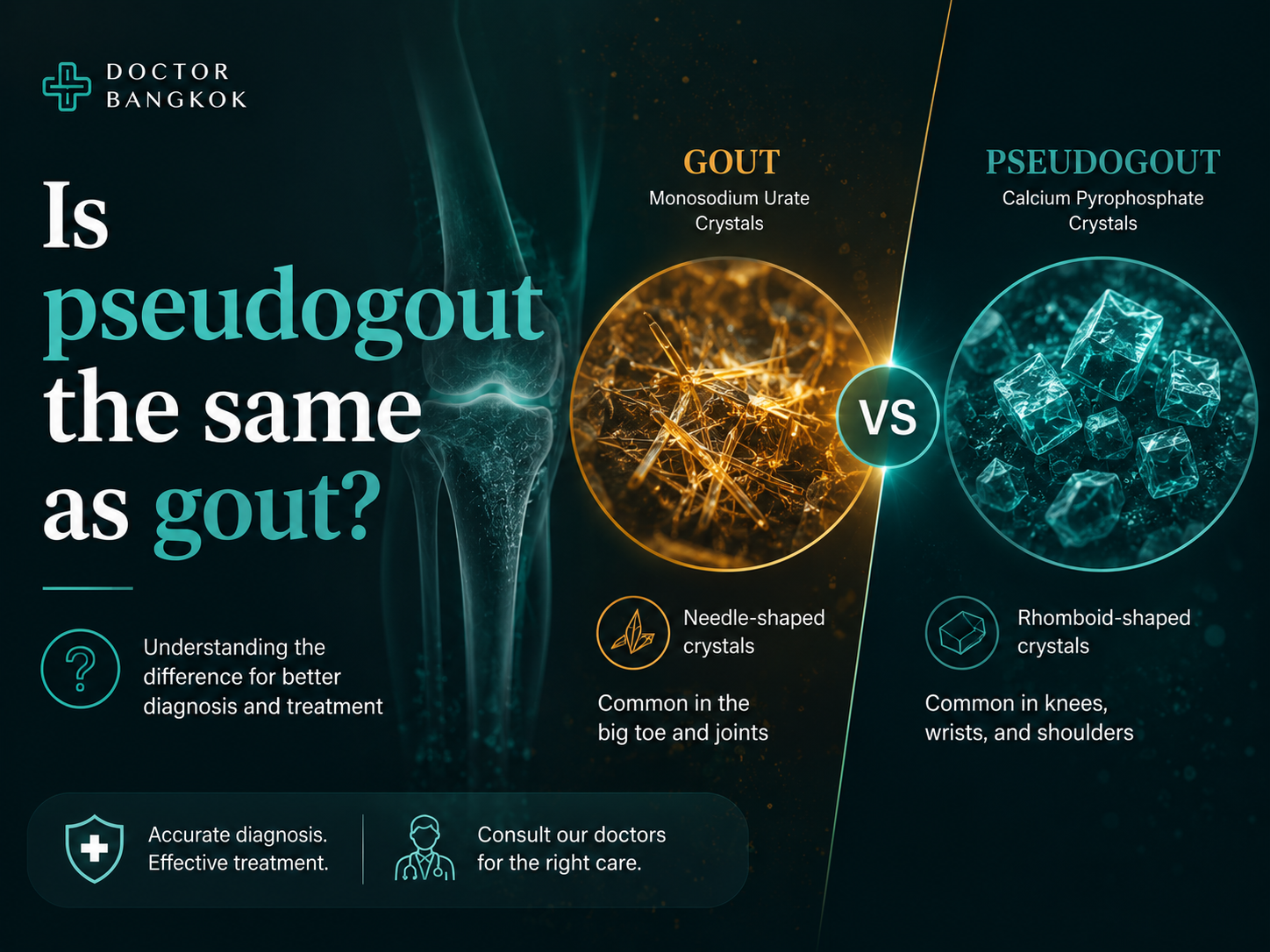
Gout is caused by uric acid crystals building up in a joint. Pseudogout is caused by a different crystal entirely, calcium pyrophosphate, sometimes called CPPD. Both types of crystals trigger the same reaction: sudden, severe joint pain, swelling, warmth, and redness that comes on fast and feels awful.
The name "pseudogout" literally means "false gout." It earned that name because it mimics gout so closely that it gets misdiagnosed regularly, even by experienced clinicians. The key differences only become clear when you look at which joint is involved, what the blood tests show, and what the crystals look like under a microscope.
Side-by-Side Comparison
| Feature | Gout | Pseudogout |
|---|---|---|
| Crystal type | Monosodium urate (needle-shaped) | Calcium pyrophosphate (rhomboid-shaped) |
| Most common joint | Big toe, ankle, foot | Knee, wrist, hip, shoulder |
| Blood test clue | High uric acid | No reliable blood marker |
| X-ray finding | Soft tissue deposits (tophi) late-stage | Calcium in cartilage (chondrocalcinosis) |
| Dietary trigger | Yes, purine-rich foods and alcohol | No dietary connection |
| Who it affects | More common in men, younger adults | More common in older adults, both sexes |
| Definitive test | Joint fluid analysis | Joint fluid analysis |
| Long-term drug option | Allopurinol (reduces uric acid) | No equivalent drug exists |

What Causes Pseudogout, and Who Gets It
Most cases of pseudogout happen in older adults, and in many patients there is no clear reason why the crystals form. Age is the biggest risk factor on its own.
Certain underlying conditions make pseudogout more likely. An overactive parathyroid gland raises calcium levels and can trigger crystal formation. Iron overload in the body, known as hemochromatosis, is another known cause. Low magnesium and an underactive thyroid have also been linked to CPPD. If you are middle-aged or younger and getting pseudogout attacks, it is worth checking for these conditions.
Gout, by contrast, is driven by high uric acid, which is often tied to diet, alcohol, kidney function, and genetics. That dietary connection does not exist for pseudogout. If you have been on a strict low-purine diet and your joint attacks continue, that is a reason to question whether gout is really the right diagnosis.
Why Your Gout Treatment May Not Be Working
I see this more often than you might expect. A patient comes in after months on allopurinol, eating carefully, avoiding alcohol, and they are still getting flares. They assume their medication is not strong enough. But sometimes the problem is simpler: they have pseudogout, not gout.
Allopurinol works by reducing uric acid. It does nothing for calcium pyrophosphate crystals. A low-purine diet will not prevent pseudogout attacks either. If you are doing everything right for gout and still suffering, the diagnosis needs to be revisited.
Both conditions can also exist at the same time in the same joint. That is uncommon, but it happens. When it does, you need treatment that covers both, and that is only possible once you know what you are dealing with.
How to Actually Tell Them Apart
A uric acid blood test is a reasonable starting point, but it is not enough on its own. Uric acid can be normal even during a genuine gout attack. And there is no blood test that confirms pseudogout.
The most reliable way to tell them apart is joint fluid analysis. A small amount of fluid is drawn from the swollen joint with a needle and examined under a microscope. Gout crystals look like fine needles. CPPD crystals look like small rhomboids, a different shape entirely. That single finding tells you exactly which condition you have.
Imaging also helps. On X-ray, CPPD leaves calcium deposits visible in the cartilage. Ultrasound can add more detail. These findings require an experienced eye to interpret correctly, and a blood test alone should never be the end of the investigation when the diagnosis is uncertain.
Getting Diagnosed in Bangkok
If you have been dealing with recurrent joint pain in Bangkok and you are not sure what you have, do not rely on a single blood test result. At Doctor Bangkok, we assess your joint clinically, run blood work including uric acid levels, and arrange imaging where needed. If joint fluid analysis is required, we will guide you through that process.
The practical problem for expats is that crystal-induced joint disease is often managed with assumptions rather than confirmed diagnoses. You deserve to know which crystal you have before committing to a treatment plan. Treating pseudogout as gout, or the other way around, wastes time and leaves you in pain.
You can read more about our approach to gout diagnosis and treatment in Bangkok and book a consultation directly through our site.
Treatment: How the Two Conditions Differ
For both conditions, the immediate goal during a flare is the same: reduce inflammation and control pain. Anti-inflammatory painkillers, colchicine, and corticosteroids all work for acute attacks of either condition. That overlap is part of why the distinction gets missed in the short term.
The difference becomes important for long-term management. For gout, allopurinol lowers uric acid and helps prevent future attacks. Dietary changes support this. For pseudogout, no equivalent long-term drug exists. Management focuses on treating flares when they happen and, if an underlying condition is found, addressing that directly.
If your pseudogout is related to hyperparathyroidism or hemochromatosis, treating those conditions may reduce how often attacks occur.
What Happens If You Leave It Untreated
With gout, repeated untreated flares allow urate deposits to build up under the skin, forming lumps called tophi. Kidney stones can also develop. These are serious but largely preventable with the right treatment started early.
With pseudogout, the long-term risk is chronic joint damage. Cartilage breaks down over time from repeated crystal-driven inflammation. This can lead to lasting loss of joint function.
Neither condition should be left unmanaged. If you have had more than one attack, the right step is a proper diagnosis and a plan, not just pain relief each time it flares.
Sudden joint swelling in Bangkok? Not sure if it is gout or something else? At Doctor Bangkok, we see this regularly and we know how to work it up properly. We offer blood tests, clinical joint assessment, imaging referrals, and guidance on next steps, all in English, in central Bangkok, with no long waits. Book a consultation at doctorbangkok.co.th or visit our gout treatment page to find out more.
Frequently Asked Questions
Can a blood test tell the difference between gout and pseudogout?
A uric acid blood test can support a gout diagnosis, but it is not conclusive on its own, and there is no blood test that confirms pseudogout. The definitive answer comes from examining joint fluid under a microscope. The crystal shape tells you exactly which condition you have.
If my gout medication is not working, could I have pseudogout instead?
Yes, and this is something I see regularly at the clinic. Allopurinol and a low-purine diet have no effect on calcium pyrophosphate crystals. If you are doing everything right for gout and still flaring, the diagnosis needs to be re-examined before you try stronger medications.
Is pseudogout related to diet the way gout is?
No. Gout is driven by purine-rich foods and alcohol raising uric acid levels. Pseudogout has nothing to do with what you eat. If you have been avoiding shellfish and beer for months and your joint attacks continue, diet is not the problem and pseudogout should be considered.
Which joints does pseudogout affect, and how is that different from gout?
Gout most commonly starts in the big toe joint. Pseudogout tends to hit the knee, wrist, hip, or shoulder. If your painful swollen joint is not in your foot, pseudogout moves up the list of possibilities. Both conditions can affect one or several joints during a single attack.
Can gout and pseudogout occur at the same time?
Yes, though it is uncommon. Both crystal types have been found in the same joint at the same time. When that happens, treating only one condition will not fully resolve your symptoms, which is exactly why joint fluid analysis matters more than assumptions.
What does treatment look like for a pseudogout flare?
During an acute flare, anti-inflammatories, colchicine, or a short course of steroids can bring the pain and swelling down quickly. The same approach works for gout flares, which is part of why the two get confused. The difference is what comes next: gout has long-term drug options to reduce future attacks, and pseudogout currently does not.
Dr. Ponlawat Pitsuwan
Physician, Doctor Bangkok
a private medical clinic in central Bangkok. He sees expats, residents, and medical tourists for joint pain, inflammatory conditions, general medical assessment, and a wide range of acute and chronic health concerns. His focus is straightforward, evidence-based care delivered in plain language.

Dr. Ponlawat Pitsuwan is a physician at Doctor Bangkok, a private clinic in central Bangkok. He sees expats, residents, and medical tourists for general medicine, wellness consultations, and IV therapy. His focus is straightforward, evidence-based care delivered in plain language.